
- Development Impact Bond
- Health and wellbeing
- Poverty reduction
- Homelessness
- Africa
Democratic Republic of Congo, Nigeria, Mali
6 mins
Humanitarian Impact Bond
Last updated: 27 Feb 2023
The aim of the humanitarian impact bond was to expand and improve the efficiency of physical rehabilitation services to people that have a physical disability and require a mobility device.
Project Location
Aligned SDGs

INDIGO Key facts and figures
-
INDIGO project
-
Commissioner
-
Intermediary
-
Investor
-
Provider
-
Evaluator
- Philanthropy Associates
-
Launch date
July 2017
-
Start of service provision
July 2017
-
Capital raised (minimum)
USD 19.70m
-
Service users
3k+
Target population
Individuals with physical disabilities in living in Mali, Nigeria, and the Democratic Republic of Congo, who are victims of war, natural disasters, congenital impairments or disabling diseases such as polio.
The problem
Across the world, 90 million people have a physical disability and require a mobility device. However, only 10% have access to adequate physical rehabilitation support. Without these services, living with a physical disability can put someone at greater risk of societal exclusion and act as a barriers to accessing education or employment.
Organisations such as the International Committee of the Red Cross (ICRC) support provision of such services, yet funding challenges are significant and operations are stretched across dozens of countries. This makes innovating and scaling new management approaches difficult.
The solution
The ICRC sought to expand and improve efficiency of physical rehabilitation services. With national government agencies and a major foundation from an international bank – La Caixa Foundation taking on the role of commissioners of support services they had a starting point.
After two years of planning, the humanitarian impact bond (HIB) launched in September 2017. This would become known as the Programme for Humanitarian Impact Investment (PHII) and it is based on the development impact bond (DIB) model. PHII secured 5 years of funding from private investors.
Using an impact bond allows the International Committee of the Red Cross to innovate and improve efficient delivery of rehabilitation services, while still ensuring high quality and well-targeted services are provided. This was done through implementing the Physical Rehabilitation Program (PRP). The primary outcome of the PHII was to increase the efficiency of these new centres compared to the historic average of comparable centres, and support at least 3,600 people to regain their mobility over two years of operations, between 2020 and 2022.
Three new Physical Rehabilitation Program centres in Mali (Mopti), Nigeria (Maiduguri) and the Democratic Republic of Congo (Kinshasa) were created. Each centre is owned and operated by a local partner with the ICRC providing support. Each centre supports communities with limited social safety nets, where people with physical disabilities risk of receiving insufficient or inadequate treatment.
These centres also serve as the location of development for a new “Digital Centre Management System”, an ICT tool that allows the management of most aspects of a Physical Rehabilitation Center. It's been developed within the framework of the PHII and is part of the measures to improving efficiency across all 107 Physical Rehabilitation Program centres. The aim here was to enable more people to receive support and rehabilitation with the same resources.
The impact
Over 3,000 persons with disability have benefited from physical rehabilitation services in the Democratic Republic of Congo (DRC), Mali and Nigeria. Despite COVID-19, military coups and peaks of violence making the implementation of the project complex, the rehabilitation centres are 9% more efficient than the benchmark centre in terms of time management, staff member skills, management of stock and resources.
Source: International Committee of the Red Cross. (2022). First Humanitarian Impact Bond successfully brings physical rehabilitation services to conflict-affected communities
Outcomes framework
The outcome payments for PHII were based on the construction of the new facility and improved mobility achieved by disabled persons receiving support. Note – the construction of the new facility is actually an output rather than an outcome, but we will use their terminology for this case study.
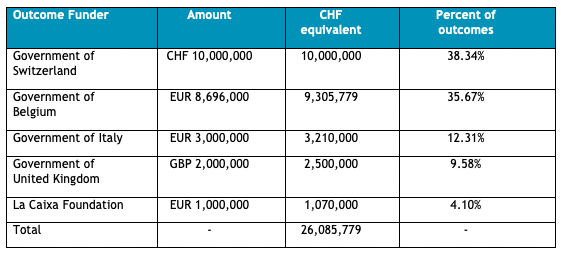
In July 2020, La Caixa Foundation was expected to pay CHF1.07 million (US$1.8 million) to investors following the construction and operationalisation of the three new rehabilitation centres in Mali, Nigeria and the Democratic Republic of Congo. La Caixa Foundation is only involved financially in this part of the outcomes framework.
In July 2022, the rest of the project commissioners were expected to pay up to CHF25 million (US$26.5 million) to investors. Repayment was based on the number of people (re)gaining mobility per rehabilitation professional at the centre (staff efficiency ratio). Investors only received a positive return on investment if the new rehabilitation centres' staff efficiency ratio exceeds the baseline average of comparable centres.
Up to 40% of investor capital was at risk, implying that investors lose 40% of their upfront investments if no outcomes were achieved. If no outcomes were achieved this means that the new rehabilitation centres were not delivering services at all, i.e. the staff efficiency ratio reached 0% of the baseline average. Outcome payments were to increase in line with the improvements in the staff efficiency ratio relative to the baseline average. Interest payments were capped at 7% internal rate of return. Each commissioner (outcome funder) was liable for a different portion of repayments to investors, summarised in the below table.
Outcome data was self-reported by the International Committee of the Red Cross across the three new rehabilitation centres and was verified by an independent auditor (Philanthropy Associates). The auditor visited a 5% sample to confirm (re)gained mobility of disabled persons who received support from the new rehabilitation centres. The International Committee of the Red Cross continued monitoring patient outcomes using participant exit surveys and video recording of mobility tests. Feedback using SMS technology was also considered.
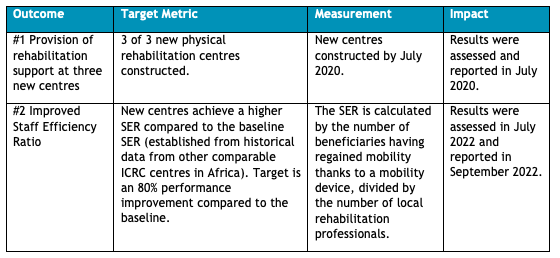
The table below summarises the project’s outcomes metrics.
Timeline
-
2015-2017
Conceptualisation of impact bond, engagement with stakeholders, design of contract
-
July 2017
Structuring completed. Intervention period begins.
-
September 2017
Public announcement.
-
July 2020
Interim results announcement and outcome payment.
-
July 2022
Intervention period ends.
-
September 2022
Final outcomes payment delivered.
Project insights
A four point rationale
This humanitarian impact bond is led by the providers – the International Committee of the Red Cross, even though there are several commissioners involved.
The ICRC's rational for implementing a DIB is four-fold, aiming to:
1) Mobilise additional resources to increase access to physical rehabilitation.
2) Test and deploy the new Digital Centre Management Tool to improve the operational efficiency of over 100 physical rehabilitation centres worldwide.
3) Expand the traditional funding base of the International Committee of the Red Cross, using a multi-year partnership involving public and private capital support.
4) Build practical knowledge about developing and implementing innovative financing structures.
Source: Alderson, H. (2018). How the first Humanitarian Impact Bond will transform financing of aid, Bond.
The third DIB to launch
The humanitarian impact bond was the third development impact bond to publicly launch and was the first to attempt to achieve outcomes in multiple countries. The two previous DIB projects have reached completion, including the Asháninka Impact Bond in Peru and the Educate Girls DIB in India.
At US$27.6 million in outcome funds, the humanitarian impact bond had more than three times the potential value of the next largest development impact bond by outcome funding – the Utkrisht Impact Bond (US$7million).
Overseas development organisations and philanthropic funders have been hesitant to use the impact bond model. However, substantial scaling of current outcome funding levels may occur through proposed outcome funds for education and elsewhere. International NGOs such as Save the Children and UNICEF are also actively exploring use of the DIB structure.
Sources: Clarke, L and Chalkidou, K (2018). Development Impact Bonds Targeting Health Outcomes – A comparative overview. Working Paper.
Incentives and innovation
Incentives and innovation may play interesting roles in achieving outcomes in the humanitarian impact bond. The ICRC has a financial incentive to achieve at least equal staff efficiency ratios in new rehabilitation centres. It has liability for repaying investors 10% of the upfront investment below achieving the baseline average staff efficiency ratio. This may heighten importance of the calculation used and centres selected for the initial baseline ratio.
Secondly, the humanitarian impact bond allows the International Committee of the Red Cross to pilot a new digital “Centre Management System”. The System could improve efficiency while maintaining quality of outcomes, in theory generating learning that will help the International Committee of the Red Cross to improve access to physical rehabilitation support across the other 100 physical rehabilitation centres that the Red Cross has in place. The system may be critical to achieving improvements in baseline outcomes for the three centres, and these improvements could create significant positive and far-reaching spillovers from the project.
Source: Alderson, H. (2018). How the first Humanitarian Impact Bond will transform financing of aid. Bond; KOIS Invest (2017) Special Edition Newsletter – Launching the world’s first Humanitarian Impact Bond with the ICRC; Department for International Development. (2018). Independent Evaluation of the Development Impact Bonds (DIBs) Pilot Programme Call Down Contract Award.
References
Communication with Jessica Cartwright, Department for International Development (DFID). October 2018
Image Credit: International Committee of the Red Cross. (2017). The world’s first “Humanitarian Impact Bond” launched to transform financing of aid in conflict-hit countries.
Africa and Middle East Education Outcomes Fund (EOF). (2018). The Education Outcomes Fund.
Alderson, H. (2018). How the first Humanitarian Impact Bond will transform financing of aid, Bond.
Avery, H. (2017). Why finance, not just aid, is the key to dealing with humanitarian crises’, Euromoney. London: Euromoney Institutional Investor PLC.
Belt, J., Kuleshov, A. and Minneboo, E. (2017). Development impact bonds: learning from the Asháninka cocoa and coffee case in Peru, Enterprise Development and Microfinance. Practical Action Publishing, 28 (1–2), pp. 130–144.
Clarke, L and Chalkidou, K. (2018). Development Impact Bonds Targeting Health Outcomes – A comparative overview. Working Paper.
Convergence, Palladium and Bertha Centre. (2018). The Utkrisht Impact Bond: Design grant case study.
Department for International Development. (2018). Independent Evaluation of the Development Impact Bonds (DIBs) Pilot Programme Call Down Contract Award
Epprecht, T. (2018). Humanitarian Impact Bond presentation at Impact Bonds Conference: Pathways to Scale
European Venture Philanthropy Initiative. (2018). Outcomes Funds in Europe.
Gustafsson-Wright, E. et al. (2017). Impact bonds in developing countries: Early learnings from the field. Brookings Institution.
International Committee of the Red Cross. (2017). The world’s first “Humanitarian Impact Bond” launched to transform financing of aid in conflict-hit countries.
ID Insight. (2018). Educate Girls Development Impact Bond, Final Evaluation Report.
KOIS Invest. (2017). Special Edition Newsletter – Launching the world’s first Humanitarian Impact Bond with the ICRC.
Relief Web. (2018). Development Impact Bonds Project Consultant (Save the Children).
UNICEF. (2018). Consultancy: Private Sector Development Impact Bond pilot, Financial Innovation Lab, Global Philanthropy, PFP.
WHO. (2011). World Report on Disability.
This case study was reviewed and last updated by Srinithya Nagarajan on September 2022
Downloads and Resources
ICRC Humanitarian Impact Bond Case Study Report
Download PDFIndependent Evaluation of the UK DFID's DIBs Pilot programme – Full Report
Download PDF